Battery technicians are exposed to work-related health risks, and their health-seeking behavior plays a critical role in determining health outcomes. This study assessed work-related health problems and health-seeking behaviors among battery technicians and office workers in Lagos State. A cross-sectional design was employed using multi-stage sampling and interviewer-administered questionnaires. Data were analyzed with SPSS version 20, and results were presented in tables. Chi-square and Fisher’s exact tests were used to determine significance at p ≤ 0.05. Battery technicians reported significantly higher rates of memory loss, drowsiness, limb numbness, constipation, and easy fatigability, as well as skin itching, breathing difficulty, sneezing, and runny nose, compared to office workers. Conversely, cough was more common among office workers. Health-seeking behaviors also differed: battery technicians were more likely to rely on chemist shops and self-medication than formal health facilities, a difference that was statistically significant. Memory loss was positively associated with years of work among technicians, while limb numbness was negatively associated with daily working hours of office workers. Easy fatigability was inversely related to technicians’ monthly income, and skin redness was negatively associated with years of work. Sneezing showed mixed associations, being negatively related to technicians’ income and office workers’ years of service but positively associated with technicians’ years of work. These findings underscore the need for targeted occupational health education, regular training, and improved access to qualified healthcare services for battery technicians. Strengthening workplace safety and promoting healthier health-seeking behaviors are essential for safeguarding this vulnerable workforce.
| Published in | Frontiers (Volume 5, Issue 4) |
| DOI | 10.11648/j.frontiers.20250504.14 |
| Page(s) | 183-192 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Battery Technicians, Occupational Health, Health-seeking Behavior, Work-related Problems
Variables | Battery technicians (n=150) | Office workers (n=150) | Test stat | df | p |
|---|---|---|---|---|---|
Age group (yrs) | |||||
21-30 | 17 (11.3) | 10 (6.7) | |||
31-40 | 47 (31.3) | 38 (25.3) | |||
41-50 | 49 (32.7) | 61 (40.7) | χ2=8.26 | 4 | 0.082 |
51-60 | 20 (13.3) | 31 (20.7) | |||
>60 | 17 (11.3) | 10 (6.7) | |||
Mean ± SD | 43.85±11.56 | 45.12±10.25 | |||
Marital status | |||||
Single | 17 (11.3) | 24 (16) | |||
Married | 126 (84.0) | 122 (81.3) | 3 | 0.111* | |
Divorced | 1 (7.0) | 3 (2.0) | |||
Separated | 6 (4.0) | 1 (0.7) | |||
Education | |||||
None | 8 (5.3) | 4 (2.7) | |||
Primary | 72 (48.0) | 46 (30.7) | |||
Secondary | 63 (42.0) | 56 (37.3) | χ2=21.53 | 3 | <0.001º |
Tertiary | 7 (4.7) | 44 (29.3) | |||
Religion | |||||
Christianity | 50 (33.3) | 84 (56.0) | |||
Islam | 100 (66.7) | 64 (42.7) | 2 | <0.001*º | |
Traditional | 0 (0.0) | 2 (1.3) | |||
Monthly income | |||||
<18,00 | 54 (36.0) | 33 (22.0) | |||
18,000 – 37,999 | 57 (38.0) | 57 (38.0) | |||
38,000 – 57,999 | 32 (21.3) | 42 (28.0) | 5 | 0.021*º | |
58,000 – 77,999 | 3 (2.0) | 12 (8.0) | |||
78,000 – 97,999 | 2 (1.3) | 4 (2.7) | |||
>98,000 | 2 (1.3) | 2 (1.3) |
General health problems | Battery workers (n=150) | Office worker (n=150) | χ2 | df | p |
|---|---|---|---|---|---|
Headache | 96 (64.0) | 98 (65.3) | 0.058 | 1 | 0.809 |
Memory loss | 56 (37.3) | 21 (14.0) | 21.402 | 1 | <0.001º |
Drowsiness | 68 (45.3) | 46 (30.7) | 6.848 | 1 | 0.009º |
Poor sleep | 38 (25.3) | 46 (30.7) | 1.058 | 1 | 0.304 |
Limb numbness | 83 (55.3) | 60 (40.0) | 7.069 | 1 | 0.008º |
Abdominal discomfort | 40 (26.7) | 34 (22.7) | 0.646 | 1 | 0.422 |
Difficulty in passing stools | 32 (21.3) | 19 (12.7) | 3.992 | 1 | 0.046º |
Urge to vomit | 19 (12.7) | 13 (8.7) | 1.259 | 1 | 0.262 |
Loss of appetite | 33 (22.0) | 28 (18.7) | 0.514 | 1 | 0.473 |
Easy fatigability | 73 (48.7) | 38 (25.3) | 17.518 | 1 | <0.001º |
Joint pain | 90 (60.0) | 96 (64.0) | 0.509 | 1 | 0.475 |
Decreased sex drive | 53 (35.3) | 40 (26.7) | 2.634 | 1 | 0.105 |
Organ-specific problemsª | |||||
Skin | |||||
Rash | 26 (17.3) | 18 (12.0) | 1.71 | 1 | 0.192 |
Itching | 39 (26.0) | 21 (14.0) | 6.75 | 1 | 0.009º |
Redness | 10 (6.7) | 9 (6.0) | 0.81 | 1 | 0.560 |
Lungs | |||||
Cough | 33 (22.0) | 51 (34.0) | 5.38 | 1 | 0.021º |
Chest tightness | 33 (22.0) | 43 (28.7) | 0.18 | 1 | 1.762 |
Breathing difficulty | 22 (14.7) | 9 (6.0) | 6.08 | 1 | 0.014º |
Nose | |||||
Sneezing | 95 (63.3) | 59 (39.3) | 17.29 | 1 | <0.001º |
Nasal itching | 20 (13.3) | 20 (13.3) | 0.00 | 1 | 1.000 |
Running nose | 82 (54.7) | 54 (36.0) | 10.55 | 1 | <0.001º |
Eyes | |||||
Redness | 57 (38.0) | 46 (30.7) | 1.79 | 1 | 0.181 |
Itching | 42 (28.0) | 43 (28.7) | 0.02 | 1 | 0.898 |
Tearing | 36 (24.0) | 32 (21.3) | 0.58 | 1 | 0.304 |
Memory loss | Battery Technician (n =150) | Office worker (n=150) | ||||||
|---|---|---|---|---|---|---|---|---|
No (n=94) | Yes (n=56) | χ2 | p | No (n=129) | Yes (n=21) | χ2 | p | |
Age group (years) | ||||||||
<40 | 37 (67.3) | 18 (32.7) | 35 (85.4) | 6 (14.6) | ||||
40-59 | 44 (57.1) | 33 (42.9) | 2.21 | 0.332 | 85 (86.7) | 13 (13.3) | 0.22 | 1.000* |
≥60 | 13 (72.2) | 5 (27.8) | 9 (81.8) | 2 (18.2) | ||||
Monthly income | ||||||||
<18,000.00 | 39 (72.2) | 15 (27.8) | 23 (79.3) | 6 (20.7) | ||||
18,000 and above | 55 (57.3) | 41 (42.7) | 3.29 | 0.070 | 106 (87.6) | 15 (12.4) | 1.34 | 0.248 |
Years of work | ||||||||
1-10 | 27 (77.1) | 8 (22.9) | 59 (84.3) | 11 (15.7) | ||||
>10 | 67 (58.3) | 48 (41.7) | 4.09 | 0.043º | 70 (87.5) | 10 (12.5) | 0.32 | 0.571 |
Daily work hours | ||||||||
0 -8 | 27 (62.8) | 16 (37.2) | 94 (88.7) | 12 (11.3) | ||||
>8 | 67 (62.6) | 40 (34.7) | 0.00 | 0.980 | 35 (79.5) | 9 (20.5) | 2.15 | 0.142 |
Limb numbness | No (n=67) | Yes (n=83) | χ2 | p | No (n=90) | Yes (n=60) | χ2 | p |
Age group (years) | ||||||||
<40 | 22 (40.0) | 33 (60.0) | 27 (65.9) | 14 (34.1) | ||||
40-59 | 37 (48.1) | 40 (51.9) | 0.84 | 0.656 | 56 (57.1) | 42 (42.9) | 0.237* | |
≥60 | 8 (44.4) | 10 (55.6) | 7 (63.6) | 4 (36.4) | ||||
Monthly income | ||||||||
<18,000.00 | 23 (42.6) | 31 (57.4) | 17 (58.6) | 12 (41.4) | ||||
18,000 and above | 44 (45.8) | 52 (54.2) | 0.15 | 0.702 | 73 (60.3) | 48 (39.7) | 0.03 | 0.866 |
Years of work | ||||||||
1-10 | 17 (48.6) | 18 (51.4) | 41 (58.6) | 29 (41.4) | ||||
>10 | 50 (43.5) | 65 (56.5) | 0.28 | 0.596 | 49 (61.2) | 31 (38.8) | 0.11 | 0.596 |
Daily work hours | ||||||||
0 -8 | 13 (30.2) | 30 (69.8) | 66 (62.3) | 40 (37.7) | ||||
>8 | 54 (50.5) | 53 (49.5) | 5.08 | 0.024º | 24 (54.5) | 20 (45.5) | 0.77 | 0.380 |
Difficulty stooling | No (n=118) | Yes (n=32) | χ2 | p | No (n=131) | Yes (n=19) | χ2 | p |
Age group (years) | ||||||||
<40 | 42 (76.4) | 13 (23.6) | 39 (95.1) | 2 (4.9) | ||||
40-59 | 63 (81.8) | 14 (18.2) | 1.08 | 0.584 | 85 (18.7) | 13 (18.2) | 0.021*º | |
≥60 | 13 (72.2) | 5 (27.8) | 7 (63.6) | 4 (36.4) | ||||
Monthly income | ||||||||
<18,000.00 | 42 (77.8) | 12 (22.2) | 23 (79.3) | 6 (20.7) | ||||
18,000 and above | 76 (79.2) | 20 (20.8) | 0.04 | 0.842 | 108 (89.3) | 13 (10.7) | 2.10 | 0.148 |
Years of work | ||||||||
1-10 | 26 (74.3) | 9 (25.7) | 65 (92.9) | 5 (7.1) | ||||
>10 | 92 (80.0) | 23 (20.0) | 0.52 | 0.470 | 66 (82.5) | 14 (17.5) | 3.62 | 0.057 |
Daily work hours | ||||||||
0 -8 | 37 (86.0) | 6 (14.0) | 94 (88.7) | 12 (11.3) | ||||
>8 | 81 (75.7) | 26 (24.3) | 1.96 | 0.162 | 37 (84.1) | 7 (15.9) | 0.59 | 0.442 |
Variable | Battery workers (n=150) | Office worker (n=150 | χ2 | df | P |
|---|---|---|---|---|---|
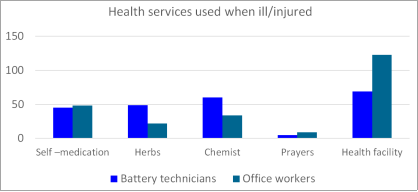
Health services used when ill/injured ªª | |||||
Self –medication | 45 (30.0) | 48 (32.0) | 0.14 | 1 | 0.708 |
Herbs | 49 (32.7) | 22 (14.7) | 14.61 | 1 | <0.001º |
Chemist | 60 (40.0) | 34 (22.7) | 11.34 | 1 | <0.001º |
Prayers | 5 (3.3) | 9 (6.0) | 0.72 | 1 | 0.395 |
Health facility | 69 (44.7) | 123 (82.0) | 42.19 | 1 | <0.001º |
Type of health facility used ª | |||||
Private | 23 (15.3) | 34 (22.7) | 41.35 | 1 | <0.001º |
Government | 43 (28.7) | 90 (60.0) | 43.46 | 1 | <0.001º |
Traditional healers’ home | 3 (2.0) | 7 (4.7) | 40.97 | 1 | <0.001º |
Health personnel at/around workplaceª | |||||
Doctor | 32 (21.3) | 116 (77.3) | 94.10 | 1 | <0.001º |
Nurse | 16 (10.7) | 27 (18.0) | 3.29 | 1 | 0.070 |
Patent medicine vendor | 50 (33.3) | 9 (6.0) | 34.47 | 1 | <0.001º |
Traditional healer | 31 (20.7) | 2 (1.3) | 28.64 | 1 | <0.001º |
Experienced co-workers | 4 (2.7) | 7 (4.5) | 0.85 | 1 | 0.357 |
None | 31 (20.7) | 0 (0.0) | 34.57 | 1 | <0.001º |
Df | Degrees of Freedom |
HBM | Health Belief Model |
HREC | Health Research Ethics Committee |
LUTH | Lagos University Teaching Hospital |
NCDC | Nigeria Centre for Disease Control |
SPSS | Statistical Package for the Social Sciences |
WHO | World Health Organization |
| [1] | Haider MJ, Qureshi N. Studies on battery repair and recycling workers occupationally exposed to lead in Karachi. Rocz Panstw Zakl Hig. 2013; 64(1): 37–42. |
| [2] | Olusegun Rasheed T. Safety Practices on Lead Poisoning Among Battery Technicians in Lagos Nigeria, 2017. Cent African J Public Heal. 2018; 4(1): 27. |
| [3] | Limits SC on OE. Recommendation from the Scientific Committee on Occupational Exposure Limits for Copper and its inorganic compounds. 2014;(January). |
| [4] | Kalahasthi RB, Barman T, Rajmohan HR. The relationship between blood lead levels and morbidities among workers employed in a factory manufacturing lead-acid storage battery. Int J Environ Present study was carried out to find Relatsh between blood lead levels Morb amongl Heal Res. 2014; 24(3): 246–55. Available from: |
| [5] | Mcneely A. A guide to India’s construction industry. ITEBuild Inter. 2015; Available from: |
| [6] | Naidana PS, Chakravarthi Burra K, Peesapati S. A study on lead toxicity among the workers in an unorganized sector of lead-acid battery industry. Al Ameen J Med Sci. 2013; 6(4): 350–5. |
| [7] |
Ahmad SA, Khan MH, Khandker S, Sarwar a FM, Yasmin N, Faruquee MH, et al. Blood lead levels and health problems of lead Acid battery workers in bangladesh. Scientific World Journal. 2014; 2014: 1–5. Available from:
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3953567&tool=pmcentrez&rendertype=abstract |
| [8] | Asampong E, Dwuma-Badu K, Stephens J, Srigboh R, Neitzel R, Basu N, et al. Health seeking behaviours among electronic waste workers in Ghana Environmental health. BMC Public Health. 2015; 15(1): 1–9. Available from: |
| [9] | Azuogu B, Eze N, Azuogu V, Onah C, Ossai E, Agu A. Appraisal of healthcare-seeking behavior and prevalence of workplace injury among artisans in automobile site in Abakaliki, Southeast Nigeria. Niger Med J. 2018; 59(5): 45. |
| [10] | Ozomata EA. Occupational Morbidities and Health-Seeking Behavior among Automobile Mechanics in the Western Region of Nigeria. 2024; 13(1): 119–28. |
| [11] | Adei D, Mensah AA, Agyemang-Duah W, Aboagye-Gyasi L. Factors associated with health-seeking behaviour among informal sector workers in the Kumasi metropolis of Ghana. Cogent Public Heal. 2022; 9(1). Available from: |
| [12] | Nwambuonwo OJ, Mughele ES. Using Geographic Information System to Select Suitable Landfill Sites For Megacities (Case Study of Lagos, Nigeria). Comput Inf Syst Dev Informatics. 2012; 3(4): 48–57. |
| [13] | Prabhakar GN. Sample size determination. Textbook of biostatistics. Jaypee Brothers Medical Publishers Ltd. Jaypee Brothers Medical Publishers Ltd; 2006. 110–19 p. |
| [14] | Sharma S, Mudgal S, Thakur K, Gaur R. How to calculate sample size for observational and experiential nursing research studies? Natl J Physiol Pharm Pharmacol. 2019; 10(0): 1. |
| [15] | Adela Y, Ambelu A, Tessema DA. Occupational lead exposure among automotive garage workers – a case study for Jimma town, Ethiopia. Vol. 7, Journal of Occupational Medicine and Toxicology. 2012. p. 15. |
| [16] | Saliu A, Adebayo O, Kofoworola O, Babatunde O, Ismail A. Comparative assessment of blood lead levels of automobile technicians in organized and roadside garages in Lagos, Nigeria. J Environ Public Health. 2015; 10: 2015. |
| [17] | Monney I, DwumfourAsare B, OwusuMensah I, Kuffour R. Occupational health and safety practices among vehicle repair artisans in an urban area in Ghana. J Environ Occup Sci. 2014; 3(3): 1. Available from: |
| [18] |
Kianoush S, Balali-Mood M, Mousavi SR, Shakeri MT, Dadpour B, Moradi V, et al. Clinical, toxicological, biochemical, and hematologic parameters in lead exposed workers of a car battery industry. Iran J Med Sci. 2013; 38(1): 30–7. Available from:
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3642942&tool=pmcentrez&rendertype=abstract |
| [19] | Assefuah Mensah S, A. Essuman M, S. Brah A, A. Aboagye P, Boye A. Assessment of Hazards, Health Consciousness and Health Seeking Behavior of Automobile Mechanics in Cape Coast Metropolis, Ghana. Sumerianz J Med Healthc. 2021;(42): 60–8. |
| [20] | Umoh MP, Amuasi JH, Jimmy AI, Tetteh MA, Opoku FA, Fallah J, et al. Knowledge, attitude and compliance to occupational health and safety practices among vehicle artisans. Quantum J Med Heal Sci. 2023; 2(1): 27–37. |
APA Style
Ozomata, E. A., Maduafokwa, B. A., Osagiede, E. F., Igwilo, U. A., Giwa, O. (2025). Work-Related Health Problems and Health Seeking Behaviour of Battery Technicians and Office Workers in Western Nigeria: A Comparative Study. Frontiers, 5(4), 183-192. https://doi.org/10.11648/j.frontiers.20250504.14
ACS Style
Ozomata, E. A.; Maduafokwa, B. A.; Osagiede, E. F.; Igwilo, U. A.; Giwa, O. Work-Related Health Problems and Health Seeking Behaviour of Battery Technicians and Office Workers in Western Nigeria: A Comparative Study. Frontiers. 2025, 5(4), 183-192. doi: 10.11648/j.frontiers.20250504.14
AMA Style
Ozomata EA, Maduafokwa BA, Osagiede EF, Igwilo UA, Giwa O. Work-Related Health Problems and Health Seeking Behaviour of Battery Technicians and Office Workers in Western Nigeria: A Comparative Study. Frontiers. 2025;5(4):183-192. doi: 10.11648/j.frontiers.20250504.14
@article{10.11648/j.frontiers.20250504.14,
author = {Ebenezer Adeiza Ozomata and Blossom Adaeze Maduafokwa and Emmanuel Friday Osagiede and Uzoamaka Allena Igwilo and Opeyemi Giwa},
title = {Work-Related Health Problems and Health Seeking Behaviour of Battery Technicians and Office Workers in Western Nigeria: A Comparative Study},
journal = {Frontiers},
volume = {5},
number = {4},
pages = {183-192},
doi = {10.11648/j.frontiers.20250504.14},
url = {https://doi.org/10.11648/j.frontiers.20250504.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.frontiers.20250504.14},
abstract = {Battery technicians are exposed to work-related health risks, and their health-seeking behavior plays a critical role in determining health outcomes. This study assessed work-related health problems and health-seeking behaviors among battery technicians and office workers in Lagos State. A cross-sectional design was employed using multi-stage sampling and interviewer-administered questionnaires. Data were analyzed with SPSS version 20, and results were presented in tables. Chi-square and Fisher’s exact tests were used to determine significance at p ≤ 0.05. Battery technicians reported significantly higher rates of memory loss, drowsiness, limb numbness, constipation, and easy fatigability, as well as skin itching, breathing difficulty, sneezing, and runny nose, compared to office workers. Conversely, cough was more common among office workers. Health-seeking behaviors also differed: battery technicians were more likely to rely on chemist shops and self-medication than formal health facilities, a difference that was statistically significant. Memory loss was positively associated with years of work among technicians, while limb numbness was negatively associated with daily working hours of office workers. Easy fatigability was inversely related to technicians’ monthly income, and skin redness was negatively associated with years of work. Sneezing showed mixed associations, being negatively related to technicians’ income and office workers’ years of service but positively associated with technicians’ years of work. These findings underscore the need for targeted occupational health education, regular training, and improved access to qualified healthcare services for battery technicians. Strengthening workplace safety and promoting healthier health-seeking behaviors are essential for safeguarding this vulnerable workforce.},
year = {2025}
}
TY - JOUR T1 - Work-Related Health Problems and Health Seeking Behaviour of Battery Technicians and Office Workers in Western Nigeria: A Comparative Study AU - Ebenezer Adeiza Ozomata AU - Blossom Adaeze Maduafokwa AU - Emmanuel Friday Osagiede AU - Uzoamaka Allena Igwilo AU - Opeyemi Giwa Y1 - 2025/12/17 PY - 2025 N1 - https://doi.org/10.11648/j.frontiers.20250504.14 DO - 10.11648/j.frontiers.20250504.14 T2 - Frontiers JF - Frontiers JO - Frontiers SP - 183 EP - 192 PB - Science Publishing Group SN - 2994-7197 UR - https://doi.org/10.11648/j.frontiers.20250504.14 AB - Battery technicians are exposed to work-related health risks, and their health-seeking behavior plays a critical role in determining health outcomes. This study assessed work-related health problems and health-seeking behaviors among battery technicians and office workers in Lagos State. A cross-sectional design was employed using multi-stage sampling and interviewer-administered questionnaires. Data were analyzed with SPSS version 20, and results were presented in tables. Chi-square and Fisher’s exact tests were used to determine significance at p ≤ 0.05. Battery technicians reported significantly higher rates of memory loss, drowsiness, limb numbness, constipation, and easy fatigability, as well as skin itching, breathing difficulty, sneezing, and runny nose, compared to office workers. Conversely, cough was more common among office workers. Health-seeking behaviors also differed: battery technicians were more likely to rely on chemist shops and self-medication than formal health facilities, a difference that was statistically significant. Memory loss was positively associated with years of work among technicians, while limb numbness was negatively associated with daily working hours of office workers. Easy fatigability was inversely related to technicians’ monthly income, and skin redness was negatively associated with years of work. Sneezing showed mixed associations, being negatively related to technicians’ income and office workers’ years of service but positively associated with technicians’ years of work. These findings underscore the need for targeted occupational health education, regular training, and improved access to qualified healthcare services for battery technicians. Strengthening workplace safety and promoting healthier health-seeking behaviors are essential for safeguarding this vulnerable workforce. VL - 5 IS - 4 ER -
Department of Community Health, Lagos University Teaching Hospital, Lagos, Nigeria;Department of Community Medicine, College of Medicine and Health Sciences, Baze University, Abuja, Nigeria
Department of Community Health, Lagos University Teaching Hospital, Lagos, Nigeria
Department of Population Health Management, Qassim Health Cluster, Buraydah, Saudi Arabia
Department of Community Health, Lagos University Teaching Hospital, Lagos, Nigeria
Department of Community Health, Lagos University Teaching Hospital, Lagos, Nigeria